
29 Jan 2024 03:44
Chapter Fourteen, part 1. Hypovolemic States
Outline
Chapter 14
- Hypovolemic States
- Etiology
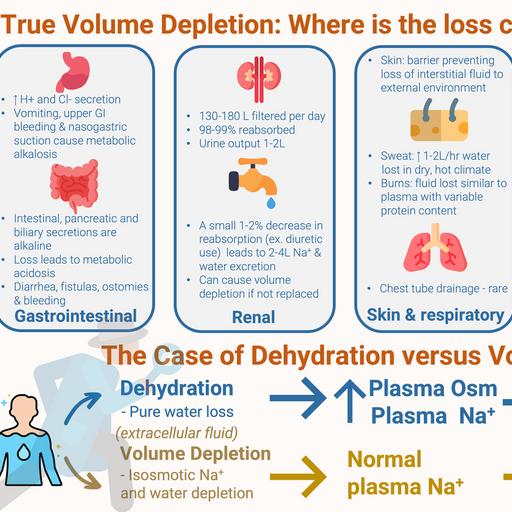
- True volume depletion occurs when fluid is lost from from the extracellular fluid at a rate exceeding intake
- Can come the GI tract
- Lungs
- Urine
- Sequestration in the body in a “third space” that is not in equilibrium with the extracellular fluid.
- When losses occur two responses ameliorate them
- Our intake of Na and fluid is way above basal needs
- This is not the case with anorexia or vomiting
- The kidney responds by minimizing further urinary losses
- This adaptive response is why diuretics do not cause progressive volume depletion
- Initial volume loss stimulates RAAS, and possibly other compensatory mechanisms, resulting increased proximal and collecting tubule Na reabsorption.
- This balances the diuretic effect resulting in a new steady state in 1-2weeks
- New steady state means Na in = Na out
- GI Losses
- Stomach, pancreas, GB, and intestines secretes 3-6 liters a day.
- Almost all is reabsorbed with only loss of 100-200 ml in stool a day
- Volume depletion can result from surgical drainage or failure of reabsorption
- Acid base disturbances with GI losses
- Stomach losses cause metabolic alkalosis
- Intestinal, pancreatic and biliary secretions are alkalotic so losing them causes metabolic acidosis
- Fistulas, laxative abuse, diarrhea, ostomies, tube drainage
- High content of potassium so associated with hypokalemia
- [This is a mistake for stomach losses]
- Bleeding from the GI tract can also cause volume depletion
- No electrolyte disorders from this unless lactic acidosis
- Renal losses
- 130-180 liters filtered every day
- 98-99% reabsorbed
- Urine output of 1-2 liters
- A small 1-2% decrease in reabsorption can lead to 2-4 liter increase in Na and Water excretion
- 4 liters of urine output is the goal of therapeutic diuresis which means a reduction of fluid reabsorption of only 2%
- Diuretics
- Osmotic diuretics
- Severe hyperglycemia can contribute to a fluid deficit of 8-10 Iiters
- CKD with GFR < 25 are poor Na conservers
- Obligate sodium losses of 10 to 40 mEq/day
- Normal people can reduce obligate Na losses down to 5 mEq/day
- Usually not a probl